The second in a series of blog posts and news items assessing the company's pivotal Phase 3 trial for unresectable locally advanced cutaneous melanoma (Stage III patients, and not metastatic [Stage IV] melanoma).
Entry 1: 3. Good or bad process:" Patient enrollment. See
Designing an interim analysis for efficacy into Provectus' pivotal melanoma Phase 3 trial
Pre-specified stopping rules based on the above types of/reasons for interim analysis(es) include:
- Safety: Stop the trial is there are x number of serious adverse events in the treatment arm (an unspecified safety stopping rule would require either a DMC or DSMB to review a trial's overall safety to make a decision to stop, if any or at all),
- Efficacy: Stop the trial for efficacy, and
- Futility: Stop the trial for futility.
* [The above, which I edited for the purposes of this blog post, essentially is copied from the March 2012 post
Futility Analysis in Clinical Trials - Stop the trial for futility of the blog
On Biostatistics and Clinical Trials]
Provectus' poster at ASCO 2015 (June) indicated the company's pivotal Phase 3 trial will have a single interim analysis for both safety and efficacy undertaken by a DMC, in addition to the trial's final data readout. Thus, the trial will be a multi-look one. Fuzzy purple emphasis below is mine.
The company also notes its interim analysis for efficacy (as well as safety) on the trial's ClinicalTrials.gov webpage. See below; fuzzy purple emphasis is mine.
PV-10 is a drug with a [very] large effect size; that is, it works very well and is far from incremental or marginal.
Provectus' ESMOR 2015 poster (September) displayed two reminders of how effective the drug is when Stage III melanoma patients have all of their disease (all their lesions) treated (i.e., injected with PV-10). At the per patient level; fuzzy purple emphasis below is mine:
At the per lesion level; fuzzy purple emphasis below is mine:
 |
| Click to enlarge. Image source is the same as immediately above |
Because of this very large effect size the pivotal trial of PV-10 for locally advanced cutaneous melanoma can withstand more than one efficacy look; that is, the additional look of an interim analysis for efficacy. Provectus, however, has not publicly discussed whether the pre-planned interim efficacy look includes a pre-specified stopping rule for efficacy. The FDA has
provided guidance regarding interim analyses for efficacy and trial stoppage that might be warranted as a result.
In order for Provectus' to seek accelerated approval on the basis of the pivotal trial's interim analysis, the beat by the PV-10 treatment arm of the chemotherapy control arm will have to be significant. In my June 2014 blog post
Trial Math: Meeting the Primary Endpoint, Pt. 1 I endeavored to calculate that hurdle rate (i.e., the size of the beat) using what information about the trial might be available. At the time and through today the company's CTO Dr. Eric Wachter, PhD has not provided the trial's hazard ratio. As a result I used a historical one Provectus' COO/CFO Peter Culpepper had publicly communicated, which facilitated the calculation of the size of the beat as 87% — PV-10's median PFS had to chemo's median PFS by 1.3 months. In the example below I used a median chemo PFS of 1.5 months, and 87% comes from the math of {(2.8 months - 1.5 months) / 1.5 months}.
 |
| Click to enlarge. |
I recently redid my clinical trial math using what appears to be a more proper and precise equation. See Suresh et al.'s (2012)
Sample size estimation and power analysis for clinical research studies, where their equation is below.
Using current parameters (such as the trial's N of 225), Eric's design yields a 90% power to detect a 70% improvement in median progression-free survival — from 1.5 months [if you use chemo's median PFS from above] to 2.55 months for PV-10. This approach also facilitates calculation, I think, of the trial's hazard ratio, which could be 0.588: {(2.55 months - 1.5 months) / 1.5 months}. By raising the hazard ratio, or lowering the size of the beat from 1.3 months {2.8 - 1.5} to ~1 month {2.55 - 1.5}, Eric may have made it easier for PV-10 to hurdle systemic chemotherapy in the trial (or made the eventual beat more impressive).
BioVex/Amgen's pivotal melanoma Phase 3 trial of OncoVEX/T-Vec for patients with advanced melanoma included a planned interim analysis for efficacy in the form of overall survival ("OS"), which was
presented at ASCO 2013. The trial's primary endpoint was durable response rate, while
OS was a secondary one that T-Vec barely missed with a p-value of 0.051.
On the other hand Vical's Allovectin-7's pivotal Phase 3 trial had no interim analysis for efficacy designed into it. See that company's CEO statement in a comment I made on a Seeking Alpha article about Vical in 2012. Fuzzy purple emphasis below is mine.
Big Pharma beats multi-efficacy look pivotal clinical trials of somewhat better drugs (i.e., having smaller effect sizes) by using large numbers of patients. The immune checkpoint inhibitors represent notable relative improvement over prior patient options; however, patient trial numbers were not insubstantial.
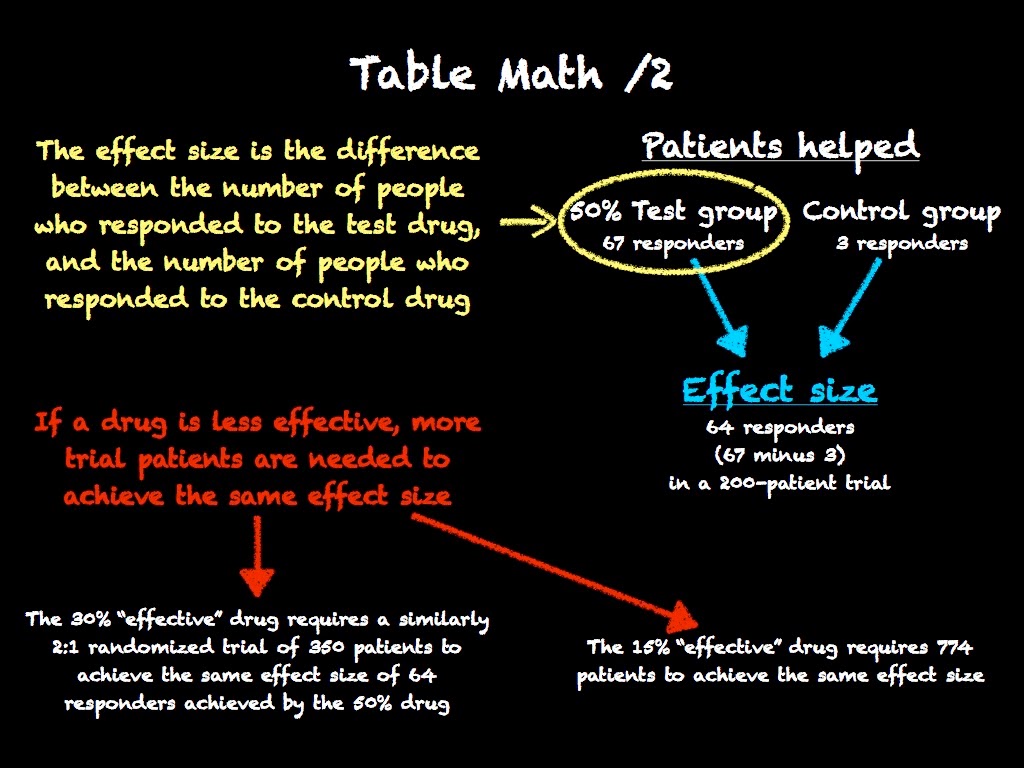
Effect size is a measure of strength (of something over something else). In the context of a clinical trial where the responses of two groups (a control group and a test drug one) are being compared, the difference in response between that of the control group and that of the test drug group is known as
the effect size.
Should the control and test (treatment) groups be close in response, and thus the test drug has a small effect (i.e., it is a less efficacious agent), a large or larger number of patients are needed in order for the test drug to distinguish itself; that is, for the confidence interval (say 90% or 95% interval) of the test drug to not overlap or run into the confidence interval of the control. Conversely, if the test drug is very effective, a large effect size may anticipated, and thus a relatively small number of trial patients are needed; that is, the confidence interval of the test arm, in this case, may be large without overlapping the confidence interval of the control arm. The fact Provectus only is utilizing 225 patients in its pivotal Phase 3 trial signals this study assumes a relatively large effect size for PV-10 (i.e., PV-10 is very efficacious). Generally speaking, the more effective a drug is the less patients would be needed (without taking into account other factors that might influence clinical trial design) in a trial.
More effective, less patients needed. Less effective, more patients needed.
Consider the spreadsheet table below, which quantifies the above discussion. In order to generate the same difference of patients helped (64 is between 62-67), the 15% "effective" drug requires a trial of 750-800 patients (774 to be precise) . The 30% "effective" drug, which is better than the 15% drug, needs 350 patients to achieve the same difference of 64 patients. The 50% "effective drug, which is better still, needs an even smaller number of patients in its trial (200).
 |
| Click to enlarge. |
The math of the above table is below.
 |
| Click to enlarge. |
 |
| Click to enlarge. |
Now see a table below I originally posted on the blog in June 2014 (note Provectus' pivotal Phase 3 trial N at the time was 210, which was later increased to 225).
 |
| Click to enlarge. |
Updating this table to include the approvals in 2014 of immune checkpoint inhibitors Keytruda and Opdivo for advanced melanoma:
- Keytruda’s efficacy was established in 173 clinical trial participants while its safety was established in 411 (source), and
- Opdivo's efficacy was demonstrated in 120 patients while its safety was evaluated in 370 (source).
 Using current parameters (such as the trial's N of 225), Eric's design yields a 90% power to detect a 70% improvement in median progression-free survival — from 1.5 months [if you use chemo's median PFS from above] to 2.55 months for PV-10. This approach also facilitates calculation, I think, of the trial's hazard ratio, which could be 0.588: {(2.55 months - 1.5 months) / 1.5 months}. By raising the hazard ratio, or lowering the size of the beat from 1.3 months {2.8 - 1.5} to ~1 month {2.55 - 1.5}, Eric may have made it easier for PV-10 to hurdle systemic chemotherapy in the trial (or made the eventual beat more impressive).
Using current parameters (such as the trial's N of 225), Eric's design yields a 90% power to detect a 70% improvement in median progression-free survival — from 1.5 months [if you use chemo's median PFS from above] to 2.55 months for PV-10. This approach also facilitates calculation, I think, of the trial's hazard ratio, which could be 0.588: {(2.55 months - 1.5 months) / 1.5 months}. By raising the hazard ratio, or lowering the size of the beat from 1.3 months {2.8 - 1.5} to ~1 month {2.55 - 1.5}, Eric may have made it easier for PV-10 to hurdle systemic chemotherapy in the trial (or made the eventual beat more impressive). Big Pharma beats multi-efficacy look pivotal clinical trials of somewhat better drugs (i.e., having smaller effect sizes) by using large numbers of patients. The immune checkpoint inhibitors represent notable relative improvement over prior patient options; however, patient trial numbers were not insubstantial.
Big Pharma beats multi-efficacy look pivotal clinical trials of somewhat better drugs (i.e., having smaller effect sizes) by using large numbers of patients. The immune checkpoint inhibitors represent notable relative improvement over prior patient options; however, patient trial numbers were not insubstantial.









No comments:
Post a Comment