 |
| Original image source |
Sometimes it takes a piece of news to (again) put things into almost complete perspective.
Consider today's press release Oncorus®, Inc. Launches with $57 Million Series A Financing. This was a topical, straightforward, sizable, early-stage (Series A) biotechnology startup company financing by notable financial (MPM) and corporate (Celgene) life sciences investors of a cancer treatment approach akin to Provectus'. The scientific basis for the company and financing (the "scientific founders," or foundation, so to speak) is the work by Drs. Joseph Glorioso III, PhD and Paola Grandi, PhD around oncolytic viruses, intralesional or intratumoral injection, and immunotherapy.
Also consider a PubMed search of "glorioso grandi." From this search, further consider, for example, (from where the basis for Oncorus may have come) Grandi et al., "Design and application of oncolytic HSV vectors for glioblastoma therapy," Expert Rev Neurother. 2009 Apr; 9(4): 505–517. Aside from improvements over injectable oncolytic viruses, it's still intratumoral injection as the route of delivery.
Updated (7/31/16): The trend towards immuno-oncology (I-O) via oncolytic virus continues — the first in this class being the October 2015 approval of Amgen's (BioVex's) talimogene laherparepvec (OncoVEXGM-CSF) — with a license transaction between Western Oncolytics and Pfizer for the former's version, this time a smallpox-related oncolytic virus: "Pfizer bags option on oncolytic virus, partners up to advance through PhI" (Nick Paul Taylor, FierceBiotech, July 29, 2016).
Gloriosio's (and Grandi's) work above, and his/their intellectual property, references the same base patent/patent application material BioVex did. See here, here (2008) and here (2011).
The scientific founder of, or the science foundation supporting, Western Oncolytics is Dr. Stephen Thorne, PhD, who comes from the same entity/organization/program — the University of Pittsburgh Cancer Institute's Cancer Virology Program — as Drs. Glorioso and Grandi. Thorne's work has been around as early as 2009 (and probably before; I have not done a thorough desk-based review of this work, but merely am observing the key details and the apparent trend): "Targeted and armed oncolytic poxviruses: a novel multi-mechanistic therapeutic class for cancer," Kirn et al., www.nature.com, January 2009.
There are several things of note to me in regards to Pfizer's involvement and certain other aspects of the deal/technology, such as: (i) no financial deal terms were announced (there's usually a reason for such); (ii) upside beyond "today" is gone; (iii) Western Oncolytics appears to only have raised a few million dollars; (iv) see the UPitt relationship/lineage above; (v) one could argue the trend is oncolytic virus, but one also could argue the trend is the tumor microenvironment (TME) as the gateway and route of delivery as the way to enter the gateway; (vi) there is no mention of Pfizer/Merck KGaA's anti-PD-L1 avelumab; (vii) more interest in the gateway, and the use of intralesional (IL) agents to enter it, and the value IL agents in combination with other therapies, especially immune checkpoint inhibitors; (viii) one could argue that Pfizer, a laggard in the immuno-oncology space, is slowing getting up to speed on where the possibility exists to catch-up (e.g., via TME, injection, oncolytic immunotherapy, etc.); and (ix) was Pfizer late again, beaten to the better UPitt oncolytic immunotherapeutic assets by Celgene and others?It also is still injection of a biologic, and therein lies the "rub." Said another way: What I know now could be what I wished I knew then. Or perhaps said even another way: An entire pharmaceutical industry unsure or unable to consider or contemplate that the injection of a chemical (Rose Bengal/PV-10/a halogenated xanthene) -- not a biologic (e.g., a Rous sarcoma virus, a herpes simplex virus, a common cold virus, a CpG oligodeoxynucleotide, an avian paramyxovirus, etc.) -- can elicit a systemic immune response.
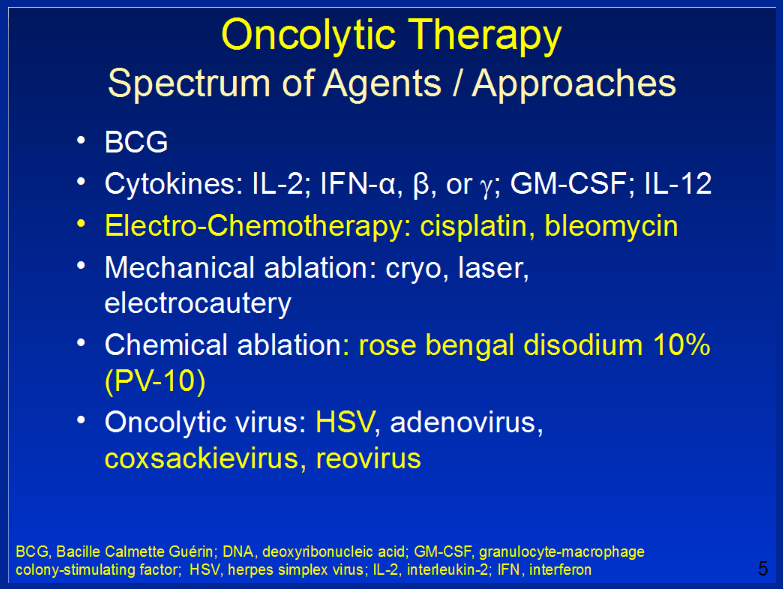
Recall St. Luke's Dr. Sanjiv Agarwala's presentation at 6th European Post-Chicago Melanoma/Skin Cancer Meeting. Setting aside Rose Bengal and chemotherapy cisplatin, I believe, everything other oncolytic agent is a biologic.
 |
| Click to enlarge. Image source |
Oncorus' algorithmic creation (by the VC MPM) and funding (by financial and corporate investors) in today's environment is proof positive the immuno-oncology space still remains wanting for a solution to vast amounts of unmet patient need, and that solution (or an important contributor to it) could be intralesional/intratumoral cancer therapy. Of course, what Oncorus is injecting is a biologic.
Provectus' data, in context, necessary and presumably sufficient to assuage the industry's concern over a [small molecule] chemical being capable of generating a systemic immune response are the results of the company's two ongoing melanoma trials, one of PV-10 as a monotherapy or single agent, and the other of PV-10 in combination with an immune checkpoint inhibitor.
Management teams, boards of directors, addressable markets, worth, valuation, etc.; those are all straightforward, and cut across industry sectors. But as a non-life sciences investor, perhaps I did not fully appreciate the apparent very high hurdle of the intralesional therapy of a small molecule chemical. Knowing what I know now, how would I have invested differently, if [I would have invested differently] at all...?
Notes:
- Rous sarcoma virus: Allovectin-7 (Vical)
- Herpes simplex virus: talimogene laherparepvec/T-Vec/Imlygic (BioVex/Amgen), HF10 (Takara Bio)
- Common cold virus: CAVATAK/Coxsackievirus (Viralytics)
- CpG oligodeoxynucleotide: SD-101 (DynaVax)
- Avian paramyxovirus (Wolchok, Allison, etc.)
No comments:
Post a Comment